Maturation of the third metacarpal
Maturation of the third proximal phalanx
BoneXpert analyses the image completely automatically, independently of the rotation of the hand. Both left and right hands are accepted.
BoneXpert analyses the following 21 bones: Radius, ulna, metacarpals, and phalanges. These are used for the overall bone age formed as a simple average over these 21 bones.
In addition, the seven carpals are considered, and a carpal bone age is computed for the group of all visible carpals. Thus the carpal bone age is not "mixed into" the overall bone age. Carpal bone age is usually not determined for boys with bone age above 12 y and for girls with bone age above 10 y, because the carpals develop very little above these bone ages.
The image analysis of the 21 bones is divided into three layers (this figure is from the first BoneXpert publication from 2009 - at that time only 13 bones were analysed, but the architecture is the same today)
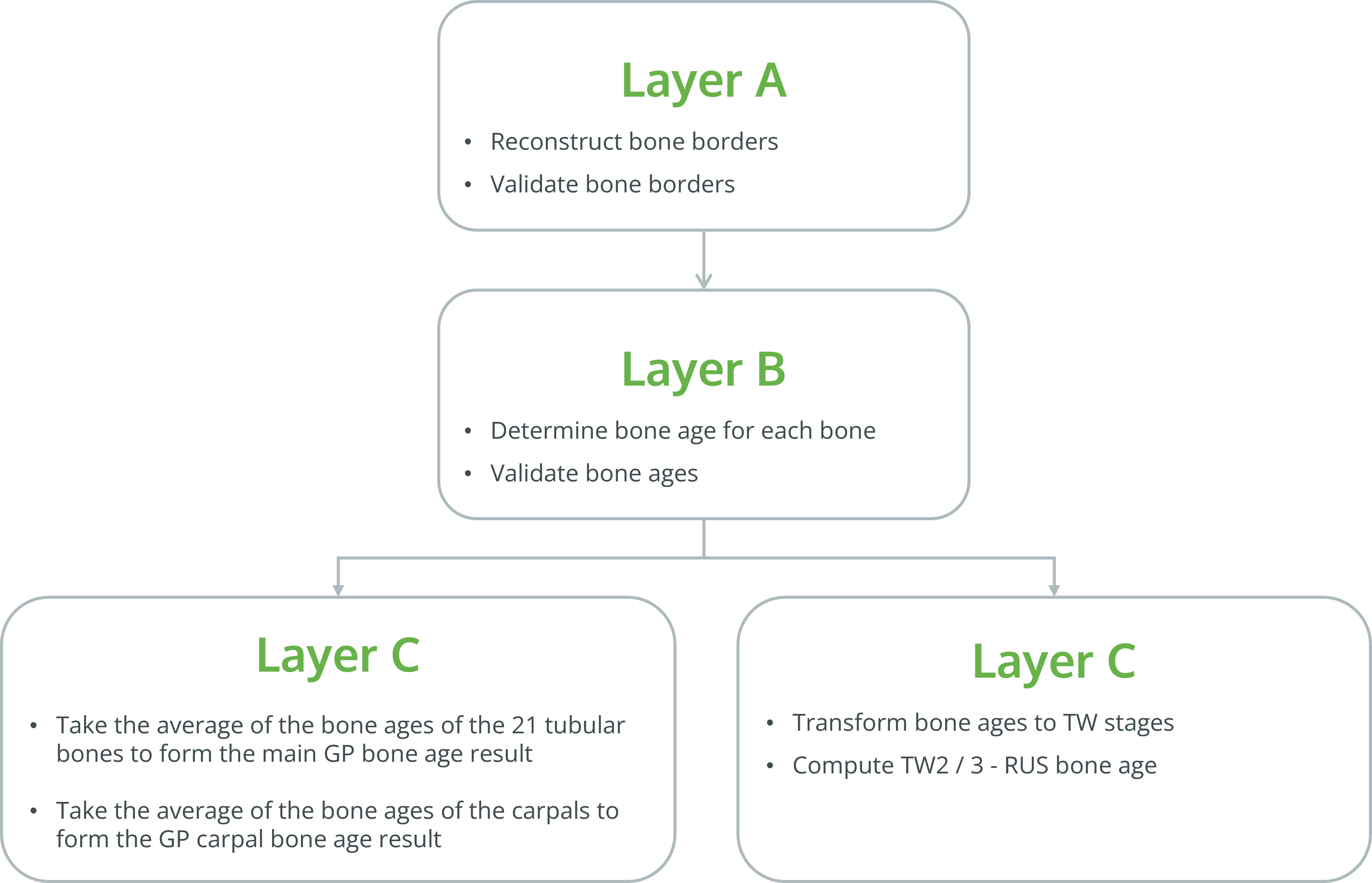
In Layer A, the borders of the bones are found using a sophisticated algorithm developed by machine learning. It is a combination of supervised and unsupervised machine learning, which has learned to locate landmarks on the bones and learned the allowed shape of each bone. This allows level A to locate each bone and reject it, if it is not in accordance with the model. A recent overview of methods of this kind can be found here. Although BoneXpert is a prominent example of artificial intelligence (AI), it differs in two ways from many recent AI methods: (1) It does not learn continuously when it runs in "production" in a hospital. (2) The image analysis is performed inside the hospital, rather than in the cloud, so the images never leave the hospital.
BoneXpert’s shape model for the third proximal phalanx of 13-17 year old boys
BoneXpert’s shape model for the third proximal phalanx of 7-13 year old boys
 The BoneXpert adult height prediction (AHP) method is a modernisation of the classical Bayley-Pinneau method from 1952.
The BoneXpert adult height prediction (AHP) method is a modernisation of the classical Bayley-Pinneau method from 1952.
Like the Bayley-Pinneau method, it is intended for normal, non-pathological untreated children
From gender, age, height and bone age, it predicts the adult height. Optionally, one can enter parental height, which improves the accuracy.
The uncertainties of the predictions of adult height are given as a standard deviation (±SD), i.e. the true values will be within the indicated range with 68% probability.
The predictor is intended to be used with Greulich-Pyle (GP) bone age determined by BoneXpert; however, it can also be used with manual GP bone age, but the uncertainties of the predictions are then considerably larger than indicated, due to the rater variability.
The tool implements the most accurate statistical model, but is not in itself a diagnostic tool, and it should not be used without consulting a pediatric endocrinologist or another medical expert.
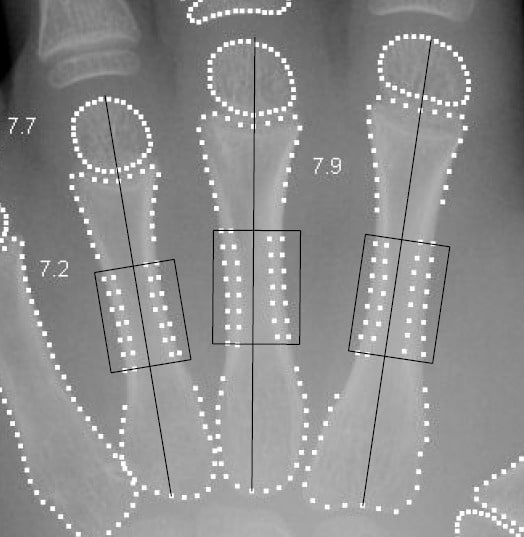
Several measures for bone health have been used in the past. Some used T directly, while others preferred the metacarpal index 2T / W, where W is the bone width. Finally, Exton-Smith used T / L, where L is the bone length.
BoneXpert’s BHI does something in between: BHI is approximately proportional to T / (LW)0.33. As explained at great length here, this formula provides the optimal compensation for the highly variable size and proportion of children.
The exact definition is BHI = π T (1 − T/W) / (LW)0.33
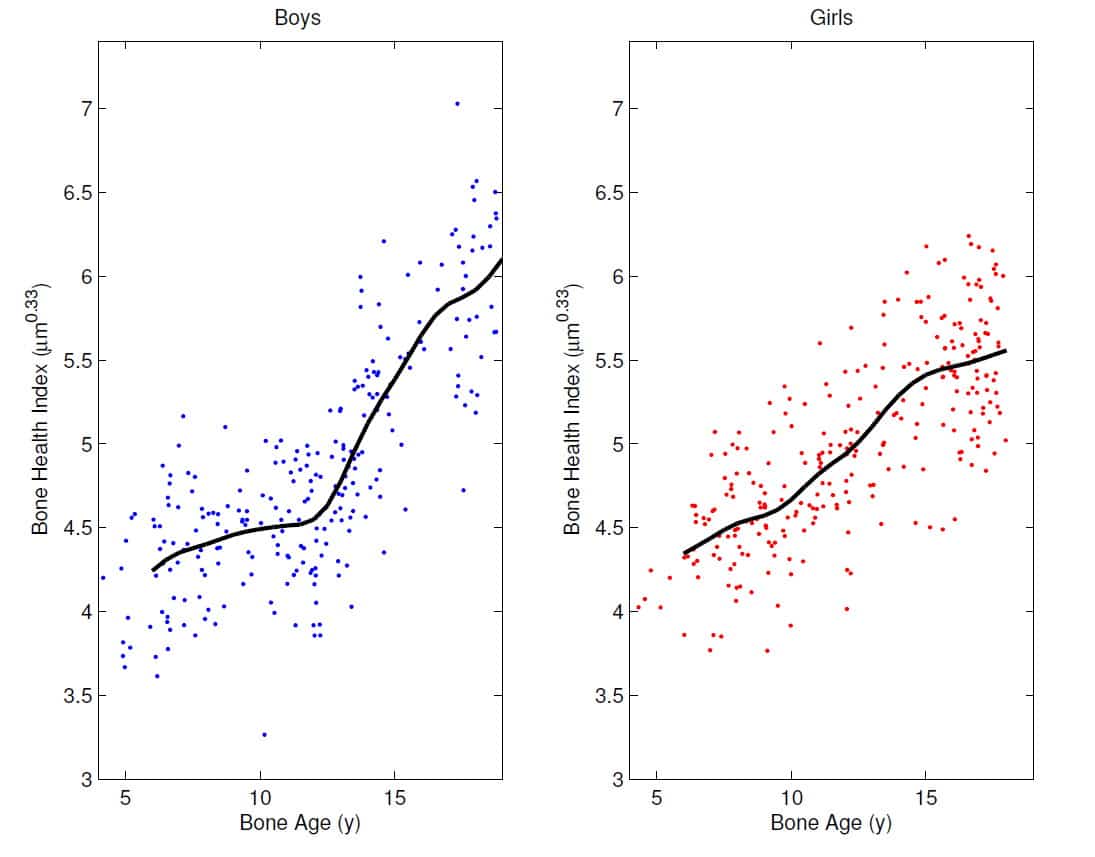
The figure above shows the BHI reference curves, i.e. the average BHI versus bone age, constructed from healthy Dutch children studied in 1997. The SD of BHI at a specific bone age is 7.5%. BoneXpert computes BHI standard deviation scores (BHI SDS) from these curves. Notice the rapid increase of BHI at puberty, illustrating the importance of assessing BHI as a function of bone age rather than age.
As a result of the large number of measurements underlying BHI, its precision (coefficient of variation, or CV) is 1.4% at age 10. The precision is the SD of results on repeated X-ray exposures, so it includes contributions from variations in the way the hand is placed on the image receptor. Since the standard deviation of BHI at fixed bone age is 7.5%, this CV corresponds to a precision of 0.19 units of BHI-SDS.
In 2019 BoneXpert's age range was extended down to neonates, and the full BHI reference curves are shown here.

In growth hormone-deficient children, it was found that BHI-SDS increases on average 0.74 units in the first year of treatment, which means that this change can be readily measured in the individual child (see DD Martin, C Heckmann, MB Ranke, G Binder, HH Thodberg, Differentiation of GH effects on metacarpal bone in children with GHD, ICCBH5, Cambridge, UK. June 23-26, 2009 Bone, Volume 45, Page S60)
BoneXpert automatically rejects the BHI determination if the bones are reconstructed inconsistently, or if the image quality is poor, e.g. due to blur of lack of contrast.